
Imagine a future where a patient’s own immune cells are reprogrammed to become super-soldiers, capable of hunting down and destroying cancer with unprecedented precision. This isn’t science fiction; it’s the reality of **what is CAR-T technology**, a revolutionary form of immunotherapy that has fundamentally reshaped the landscape of cancer treatment. As of 2026, CAR-T cell therapy stands as a beacon of hope, particularly for patients battling certain aggressive blood cancers who have exhausted other treatment options. This comprehensive guide will delve deep into the intricacies of CAR-T technology, exploring its mechanisms, applications, challenges, and future potential.
Key Takeaways
- CAR-T technology involves genetically engineering a patient’s own T-cells to express Chimeric Antigen Receptors (CARs), enabling them to specifically target and destroy cancer cells.
- It represents a highly personalized and potent form of immunotherapy, primarily approved for specific blood cancers like certain lymphomas, leukemias, and multiple myeloma.
- The process includes T-cell collection, genetic modification, expansion, and re-infusion, followed by close monitoring for potential, sometimes severe, side effects like Cytokine Release Syndrome (CRS) and neurotoxicity.
- Significant advancements are ongoing in 2026, with research focusing on expanding CAR-T applications to solid tumors, improving safety profiles, and enhancing accessibility.
- Despite its transformative potential, CAR-T therapy faces challenges related to manufacturing complexity, high cost, and the management of unique side effects.
Understanding What is CAR-T Technology: The Basics
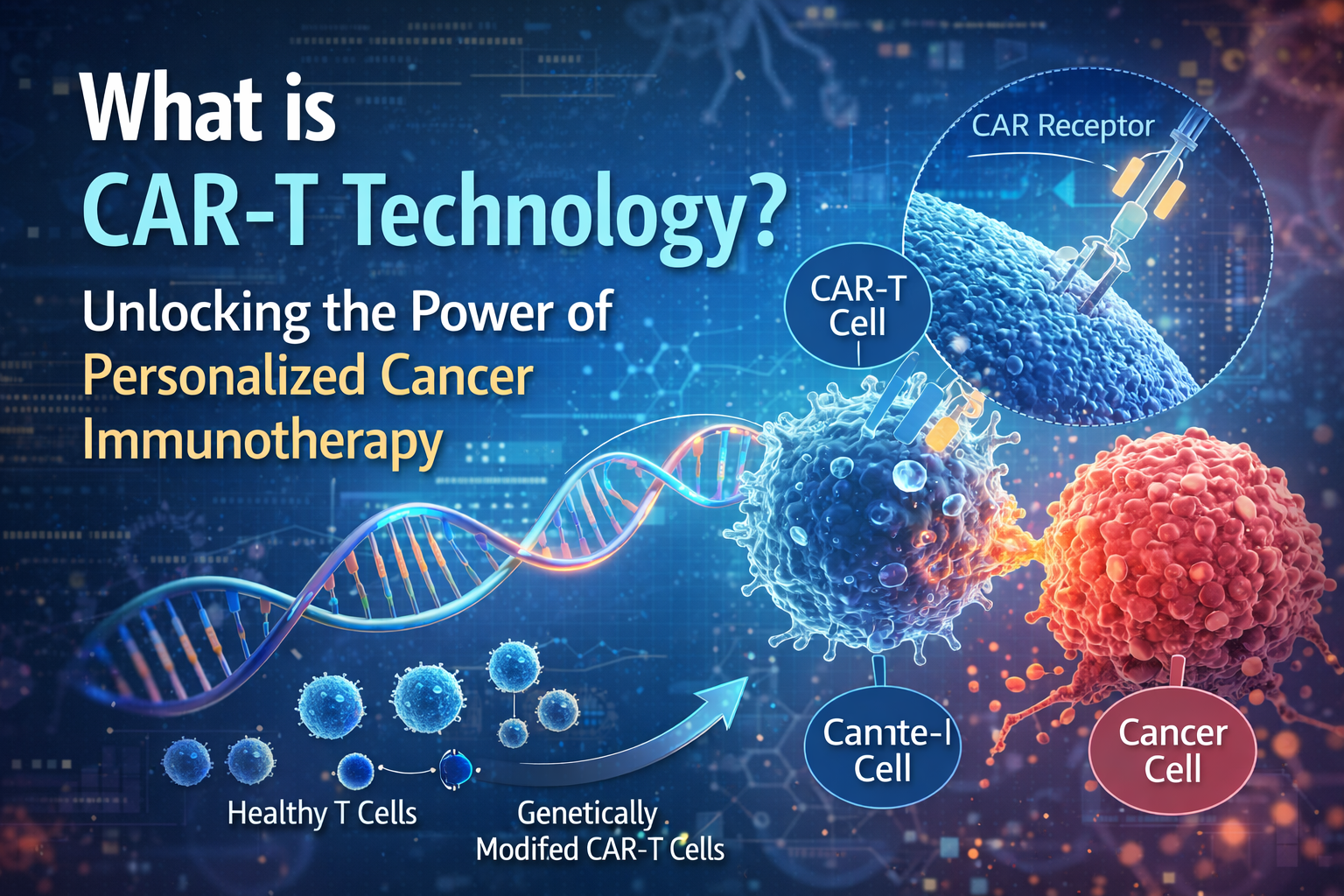
At its core, CAR-T technology, short for Chimeric Antigen Receptor T-cell therapy, harnesses the body’s natural defense system – the immune system – to fight cancer. Specifically, it uses T-cells, a type of white blood cell crucial for immune responses, and equips them with enhanced cancer-fighting abilities. Unlike traditional chemotherapy or radiation, which can harm healthy cells alongside cancer cells, CAR-T therapy is designed to be highly specific [1].
What is a Chimeric Antigen Receptor (CAR)? 🤔
The “CAR” in CAR-T is the lynchpin of this technology. A Chimeric Antigen Receptor (CAR) is a synthetic receptor that scientists engineer and introduce into T-cells. Think of it as a specially designed “GPS” system for the T-cell. Normal T-cells recognize invaders like viruses or bacteria through their natural T-cell receptors, which require cancer cells to present specific markers via MHC (Major Histocompatibility Complex) molecules. Cancer cells often cleverly evade this recognition. The CAR, however, bypasses this limitation. It is designed to directly recognize and bind to a specific protein (antigen) found on the surface of cancer cells, independent of MHC [2].
Defined Term: Chimeric Antigen Receptor (CAR)
A synthetic receptor engineered to be expressed on the surface of T-cells. CARs are designed to recognize and bind to specific antigens on cancer cells, enabling the T-cells to target and destroy the cancer cells independently of major histocompatibility complex (MHC) presentation.
The Journey of CAR-T Technology: A Step-by-Step Process
The creation and administration of CAR-T cell therapy is a complex, multi-stage process that typically spans several weeks. Understanding this journey is key to grasping the full scope of what is CAR-T technology.
| Stage | Description | Timeline (Approx.) |
|---|---|---|
| 1. T-Cell Collection (Apheresis) | Patient’s blood is drawn, and T-cells are separated using a machine. | 4-6 hours |
| 2. Genetic Engineering | T-cells are sent to a lab, where a new gene (for the CAR) is inserted. | 1-2 days (lab process) |
| 3. CAR-T Cell Expansion | The modified CAR-T cells are multiplied to millions. | 2-3 weeks |
| 4. Conditioning Chemotherapy | Patient receives chemotherapy to prepare their body for the new cells. | 3-5 days before infusion |
| 5. CAR-T Cell Infusion | The personalized CAR-T cells are infused back into the patient. | ~30 minutes |
| 6. Monitoring & Recovery | Close observation for side effects and effectiveness. | Weeks to months post-infusion |
Detailed Steps of the CAR-T Cell Therapy Process
-
T-Cell Collection (Apheresis) 🩸
The journey begins with apheresis, a procedure similar to donating blood. The patient’s blood is drawn, and a specialized machine separates the T-cells from other blood components, which are then returned to the patient. This ensures a supply of the patient’s own, unique immune cells [3].
-
Genetic Engineering in the Lab 🧬
Once collected, the T-cells are sent to a highly specialized manufacturing facility. Here, scientists use a viral vector (often a lentivirus or retrovirus, rendered harmless) to deliver a new gene into the T-cells. This gene contains the blueprint for the Chimeric Antigen Receptor. The T-cells effectively become “reprogrammed” to express this CAR on their surface.
-
CAR-T Cell Expansion 📈
The genetically modified CAR-T cells are then cultured and expanded in the lab. This crucial step increases their numbers from a relatively small initial sample to hundreds of millions, ensuring a potent therapeutic dose. This expansion phase typically takes several weeks.
-
Conditioning Chemotherapy (Lymphodepletion) 🧪
Before the CAR-T cells are infused back into the patient, a short course of chemotherapy is often administered. This “lymphodepleting” chemotherapy serves two main purposes: it reduces the patient’s existing immune cells, creating space for the newly introduced CAR-T cells to multiply, and it can also suppress regulatory T-cells that might otherwise dampen the CAR-T cell response [4].
-
CAR-T Cell Infusion 💉
Finally, the expanded and potent CAR-T cells are infused back into the patient, much like a standard blood transfusion. Once in the bloodstream, these reprogrammed cells begin their mission: to locate, bind to, and destroy cancer cells expressing the target antigen.
-
Monitoring and Management of Side Effects 🏥
Patients typically remain hospitalized or under very close medical supervision for several weeks after infusion. This is critical for monitoring and managing potential side effects, which can be severe but are generally manageable when detected early. We will explore these side effects in detail later.
Current Applications of What is CAR-T Technology in 2026
As of 2026, CAR-T technology has achieved significant breakthroughs, primarily in the treatment of certain hematological (blood) cancers. These therapies offer a lifeline to patients who have failed multiple prior treatments, often achieving durable remissions previously thought impossible [5].
The main approved indications for CAR-T cell therapies currently include:
- Relapsed/Refractory B-cell Acute Lymphoblastic Leukemia (ALL): Primarily for children and young adults.
- Relapsed/Refractory Large B-cell Lymphoma (LBCL): Including diffuse large B-cell lymphoma (DLBCL), primary mediastinal large B-cell lymphoma (PMBCL), and follicular lymphoma transformed to DLBCL, in adults.
- Relapsed/Refractory Mantle Cell Lymphoma (MCL): For adult patients.
- Relapsed/Refractory Follicular Lymphoma (FL): In adult patients after two or more lines of systemic therapy.
- Relapsed/Refractory Multiple Myeloma (MM): A significant advancement for this plasma cell disorder.
These therapies are typically reserved for patients who have relapsed after or are refractory to other standard treatments, positioning CAR-T as a powerful option in later lines of therapy. The targets for these approved therapies are usually CD19 (for B-cell malignancies) or BCMA (for multiple myeloma), antigens commonly expressed on these cancer cells.
Side Effects and Management in CAR-T Therapy
While remarkably effective, CAR-T therapy is not without its risks. The powerful immune response it unleashes can lead to unique and potentially severe side effects. Understanding these is crucial for anyone considering or managing **what is CAR-T technology**.
Related Posts:
- What is Neuralink Technology? Unlocking the Brain's…

- What Is Modern Agriculture Technology Innovations in Farming

- What Is Automation Engineering Technology The Future…

- How Does Infrared Technology Work Sensing Heat and Data

- What Is a Technology Application Software and Tools…

- How to Get Into Health Information Technology A…

-
Cytokine Release Syndrome (CRS) 🔥
CRS is the most common and often the most severe side effect. It occurs when the activated CAR-T cells release a flood of inflammatory molecules called cytokines into the bloodstream. This systemic inflammation can affect various organs and cause symptoms ranging from fever, fatigue, and muscle aches to more severe manifestations like hypotension (low blood pressure), hypoxia (low oxygen), and organ dysfunction (cardiac, renal, hepatic). CRS is graded by severity, and severe cases require intensive care and specific medications like tocilizumab (an IL-6 receptor blocker) and corticosteroids [6].
-
Immune Effector Cell-Associated Neurotoxicity Syndrome (ICANS) 🧠
ICANS is another significant concern, affecting the brain and nervous system. Symptoms can include confusion, delirium, expressive aphasia (difficulty speaking), tremors, seizures, and even cerebral edema (brain swelling). Like CRS, ICANS is graded, and management often involves corticosteroids and supportive care. The exact mechanisms linking CAR-T activation to neurotoxicity are still being researched [7].
-
Other Potential Side Effects
Less common but possible side effects include:
- Hypogammaglobulinemia: Low levels of antibodies, increasing infection risk.
- Prolonged Cytopenias: Low blood cell counts (platelets, neutrophils) that can persist for weeks or months.
- Infections: Due to immune suppression from lymphodepleting chemotherapy and the therapy itself.
- Tumor Lysis Syndrome: Occurs when cancer cells die rapidly, releasing their contents into the blood.
Due to the potential for serious side effects, CAR-T cell therapy is administered and managed in highly specialized centers with experienced multidisciplinary teams.
Challenges and Limitations of What is CAR-T Technology
Despite its groundbreaking success, CAR-T technology faces several significant challenges that limit its broader application and accessibility.
Manufacturing Complexities and Cost 💸
The personalized nature of CAR-T therapy means that each dose is custom-made for a single patient, starting with their own cells. This bespoke manufacturing process is incredibly complex, time-consuming, and expensive. The high cost of CAR-T treatments, often hundreds of thousands of dollars per patient, presents a major barrier to access globally and strains healthcare systems [8].
Accessibility Issues 🌍
Due to the specialized infrastructure required for manufacturing, administration, and managing side effects, CAR-T therapy is only available at a limited number of certified treatment centers. This poses significant logistical and financial burdens for patients who may need to travel far from home to receive treatment, further exacerbating inequities in access.
Efficacy in Solid Tumors 💪 (Ongoing Research)
While highly effective in certain blood cancers, CAR-T therapy has shown limited success against solid tumors (e.g., lung, breast, colon cancer). Several factors contribute to this:
- Antigen Heterogeneity: Solid tumors often have a more diverse mix of cancer cells, some of which may not express the target antigen, allowing them to escape.
- Immunosuppressive Tumor Microenvironment: Solid tumors often create a hostile environment that suppresses immune cell activity, making it difficult for CAR-T cells to penetrate and persist.
- Physical Barriers: Solid tumors can have dense extracellular matrices that physically impede CAR-T cell infiltration.
Potential for Relapse 🔄
Even with successful initial responses, some patients may relapse. This can occur if cancer cells lose the target antigen (antigen escape) or if the CAR-T cells lose their persistence or function over time.
The Future of CAR-T Technology in 2026 and Beyond
The field of CAR-T technology is evolving rapidly. As of 2026, extensive research and development are underway to overcome current limitations and expand the reach of this powerful therapy.
Expanding to Solid Tumors
�
�
Researchers are exploring novel strategies to enhance CAR-T cell efficacy against solid tumors. These include:
- Identifying new tumor-specific antigens: Searching for targets unique to solid tumors.
- “Armored” CAR-T cells: Engineering CAR-T cells to secrete additional molecules (e.g., cytokines) that overcome the immunosuppressive tumor microenvironment [9].
- Regional delivery: Administering CAR-T cells directly into or near the tumor site to improve penetration.
- Dual-targeting CARs: Designing CAR-T cells to target two different antigens simultaneously to prevent antigen escape.
Improving Safety and Reducing Side Effects ✅
Efforts are focused on developing “smarter” CAR-T cells with built-in safety switches that can be activated to turn off the cells if severe side effects occur. Other strategies include fine-tuning the CAR design to reduce off-target toxicity and optimizing lymphodepleting regimens.
“Off-the-Shelf” Allogeneic CAR-T Cells 📦
Currently, CAR-T therapy is autologous (using the patient’s own cells). Allogeneic CAR-T cells, derived from healthy donors, are being investigated as an “off-the-shelf” option. This could significantly reduce manufacturing time and cost, making the therapy more readily available. However, challenges like graft-versus-host disease (GVHD) and rejection of the donor cells need to be addressed [10].
Enhanced Persistence and Durability 🌟
Scientists are continuously refining CAR designs and manufacturing processes to create CAR-T cells that persist longer in the body and maintain their anti-cancer activity for extended periods, aiming for more durable remissions.
New Combinations 🤝
CAR-T therapy is being explored in combination with other treatments, such as checkpoint inhibitors, radiation, or targeted therapies, to achieve synergistic effects and improve overall outcomes.
The Economic and Ethical Landscape of CAR-T Technology
The emergence of CAR-T technology has also ignited important discussions regarding its economic impact and ethical considerations.
Cost-Effectiveness and Reimbursement 💰
The high upfront cost of CAR-T therapy requires careful evaluation of its long-term cost-effectiveness, especially considering the potential for curative outcomes in some patients. Healthcare systems worldwide are grappling with how to integrate and reimburse these therapies sustainably. Value-based payment models are being explored to align payment with clinical outcomes.
Equity and Access 🤔
Ensuring equitable access to CAR-T therapy for all eligible patients, regardless of socioeconomic status or geographic location, remains a critical ethical challenge. Efforts are needed to expand the number of treatment centers, streamline the manufacturing process, and potentially reduce costs.
Informed Consent and Patient Expectations
🗣
️
Given the complexity of the therapy and the potential for severe side effects, robust informed consent processes are paramount. Patients and their families must have a clear understanding of the risks, benefits, and uncertainties associated with CAR-T treatment.

Conclusion: The Transformative Impact of What is CAR-T Technology
As we navigate 2026, it is clear that **what is CAR-T technology** represents one of the most exciting and transformative advancements in modern medicine. This personalized cellular immunotherapy has not only revolutionized the treatment of specific blood cancers but has also opened new avenues for understanding and combating cancer using the body’s own immune system. From its intricate process of T-cell reprogramming to its profound clinical impact, CAR-T therapy offers a powerful testament to human ingenuity in the face of disease.
While challenges related to cost, accessibility, and efficacy in solid tumors persist, the relentless pace of research and development promises a future where CAR-T technology is safer, more widely available, and effective against an even broader spectrum of cancers. The journey of CAR-T cells, from a patient’s blood to a lab, and back into the body as a targeted cancer killer, epitomizes the cutting edge of personalized medicine.
Actionable Next Steps for Further Learning:
- Consult an Oncologist: If you or a loved one are facing a cancer diagnosis, discuss with your oncology team whether CAR-T therapy is a suitable option based on your specific cancer type and medical history.
- Visit Reputable Medical Websites: Explore resources from organizations like the National Cancer Institute (NCI), American Cancer Society (ACS), or major academic medical centers for the latest information and clinical trial updates.
- Stay Informed on Research: The field is rapidly evolving. Keep an eye on news from medical conferences and research journals for breakthroughs in CAR-T technology, especially concerning solid tumors and novel targets.
- Support Cancer Research: Contributions to cancer research can accelerate the development of next-generation immunotherapies and make treatments like CAR-T more accessible and effective for all.
References
[1] Neelapu, S. S., et al. (2017). Axicabtagene Ciloleucel CAR T-Cell Therapy in Refractory Large B-Cell Lymphoma. New England Journal of Medicine, 377(26), 2531–2544.
[2] Sadelain, M., et al. (2017). The Promise and Potential Pitfalls of Chimeric Antigen Receptor T-Cell Therapy. Cold Spring Harbor Perspectives in Medicine, 7(6), a027952.
[3] Kochenderfer, J. N., et al. (2015). B-cell depletion and remissions of lymphoma after CD19-targeted CAR T-cell therapy. Journal of Clinical Oncology, 33(4), 540-549.
[4] Gauthier, J., et al. (2020). Lymphodepletion for CAR T cell therapy: a comprehensive review. Nature Reviews Clinical Oncology, 17(10), 614-627.
[5] June, C. H., et al. (2018). CAR T cell immunotherapy for human cancer. Science, 359(6382), 1361-1365.
[6] Lee, D. W., et al. (2014). Current concepts in the diagnosis and management of cytokine release syndrome. Blood, 124(2), 188-195.
[7] Santomasso, B. D., et al. (2019). Immune Effector Cell-Associated Neurotoxicity Syndrome (ICANS): an updated consensus grading system and management algorithm from the American Society for Transplantation and Cellular Therapy (ASTCT). Biology of Blood and Marrow Transplantation, 25(6), 1184-1191.
[8] D’Souza, A., et al. (2020). Economic considerations and value of CAR T-cell therapy. Blood Advances, 4(13), 3217-3228.
[9] Srivastava, S., & Riddell, S. R. (2018). Engineering CAR-T cells: Successes and challenges. Trends in Immunology, 39(8), 618-631.
[10] Cieri, N., et al. (2020). Allogeneic CAR T-cells: a step closer to universal cancer immunotherapy. Annals of Oncology, 31(1), 22-30.
